
|
Zhengzhou Safute Electronic Equipment Co., Ltd.
|
Product (116)
- Obstetrics and Gynecology Equipment (7)
- Anorectal Treating Device (24)
- Anorectal Treating Device Accessories (24)
- Anorectal Physical Therapy Device (9)
- Anorectal Physical Therapy Device Accessories (9)
- Colorectal Endoscope Diagnosis Equipment (6)
- Endoscope Prodcts (8)
- Disposable Medical Accessories (8)
- Disinfection Devices (6)
- Surgical Instruments (7)
- Local Anethetic Drugs (8)
Download (4)
BEIM TECH (5)
Hemorrhoids Tips (6)
News (48)
Certificates (1)
Credit Report
Products Index
Company Info
Zhengzhou Safute Electronic Equipment Co., Ltd. [China (Mainland)]
Business Type:Manufacturer, Trading Company
City: Zhengzhou
Province/State: Henan
Country/Region: China (Mainland)
Follow Us:



BEIM TECH
Preparation Before Operation
For patients who received the treatment requires natural defecation, or at the discretion of the bowel. Before the surgery ask about the disease history and the necessary checks, pay special attention to hypertension, diabetes, blood diseases, cardiac function incomplete systemic disease. Carry out necessary auxiliary examinations, such as blood and urine routine, Chest X-rays, to determine the treatment location and treatment methods.
The prepared gauze, cotton wool, suppositories, Jingwanhong etc.
Anesthesia method
Preparation of commonly used narcotic drugs:
A Lidocaine 1% 10-20ml infiltration injection
B Bupivacaine 0.25% 10-20ml infiltration injection
C Procaine hydrochloride 1% 10-20ml procaine injection
Add a little adrenaline 2-3 drops to prolong the duration of anesthesia, reduce the toxic reaction.
Configuration of long acting anesthetic
The anesthetic 3-4ml plus 1% 1ml coeruleum methylenumadd 2-3 drops of adrenaline
Procaine hydrochloride has an allergic reaction, routine skin test is necessary. In recent years, the use of local anesthesia with lidocaine, dispersion, it is fast acting. Concentration is suitable to 0.25%-0.25%, adult maximum dose does not exceed 400mg. Anorectal treatment instrument has good hemostatic effect and does not require the addition of epinephrine. Attention to case poisoning reaction, once occurred, timely rescue.
Local anesthesia operation
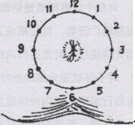
Strict aseptic operation. Although anal disease is a bacterium operation, medical personnel musttreat it asaseptic operation. Perianal skin disinfection should berange, large. Iodine, bromo-geramine, Chlorhexidine and other disinfection drugs are available. The injection site: 12 clock direction can be the first position while patient ingenucubital position .Put the needle into skin, then along this point to 3, 9clockdirection, and then by 3, 9 points to 6 points, respectively, subcutaneous infiltration anesthesia.
.
After anesthesia expand anus, anal relaxation beoreoperation.
Waist Anesthesia
The patients were placed in lateral position, back bent, knees close to the abdominal wall.
About 4-5cm up to the coccygeal tip there are two sacral cornus, then up to the middle partit isfourth sacral spine .It is a bone uplift.
In middle between two sacral cornus and fourth sacral spine there is an soft tissue depression, it issacral hiatus. And in the depths of the bony edges can touch the skin, with a fingernail do identification, routine disinfection.
With a 20ml syringe inhalation liquid, 6-6.5 needle head, through the sacral hiatus hole,put the needle into the skin with 90 degree angle with skin, releasing small amount of anesthesia while deeper and deeper.
When the needle pierced the sacral ligament tissue and fibrous tissue after tail resistance significantly plummeted a sense of frustration, that has arrived in the sacral lumen. Pumpback syringe without blood and cerebrospinal fluid inject anesthetic 20-30 ml.
.gif)
